1. Step Down (3 x 12) - Depending on the conditioning level of your patient/athlete, this can be a tricky exercise. In this specific case, considering his knee, he was placed near a wall for concerns of him falling over, or needing extra support in the event he felt instability. The athlete starts with one leg over the side of the platform, and upon partially squatting with the affixed leg, the hanging leg is to touch the ground with the heel as the only part of the foot making contact. Concurrently, in this case, the athlete mimics a chest pass with a medicine ball (see picture). The addition of the upper body movement forces the lower extremity to work more towards balancing the whole body.


2. Step Ups (6 x 30 secs) - A commonly used exercise designed to build confidence, speed, coordination, and explosion. This can be progressed in variety of ways from changing the height of the steps, to increasing the duration of the exercise, and adding a combination of toe-touches alternating one foot, to two foot sets, etc. You will find with athletes, they love to be challenged and rewarded, so adding various contests may help them to strive.


3. Drag Squats (5 x each direction) - This is an original exercise performed in three planes; forward, laterally, and "open," which is similar to a reverse lunge, except there is 45 degree rotation in the hips along the vertical axis. Pictured below is an example of a lateral drag squat. Once the player is in start position, they are to lunge out as far as they can tolerate, and from there, drag their foot back to the beginning position. This can be performed with, or without, a medicine ball.

4. Alternate Dead Lifts (3 x 15) - This exercise is performed slowly with the athlete essentially placing the dumbbell on the ground, and then lifting it up, and switching to the other side. It is hard to perform without involving hip flexion, but the only movement should be occurring at the knee. Progress the exercise by adding heavier weight, increasing duration, reps/sets, etc.


5. Hill Climbers (6 x 30secs) - A familiar exercise among athletes who condition or strength train, this variation involves the use of the Dynadisc which secondarily works the upper body, and provides more of an overall challenge. Make sure to recognize if the athlete is driving their knees up and in, and not outward, and also are not bouncing their butts, meaning their back should be mostly flat.


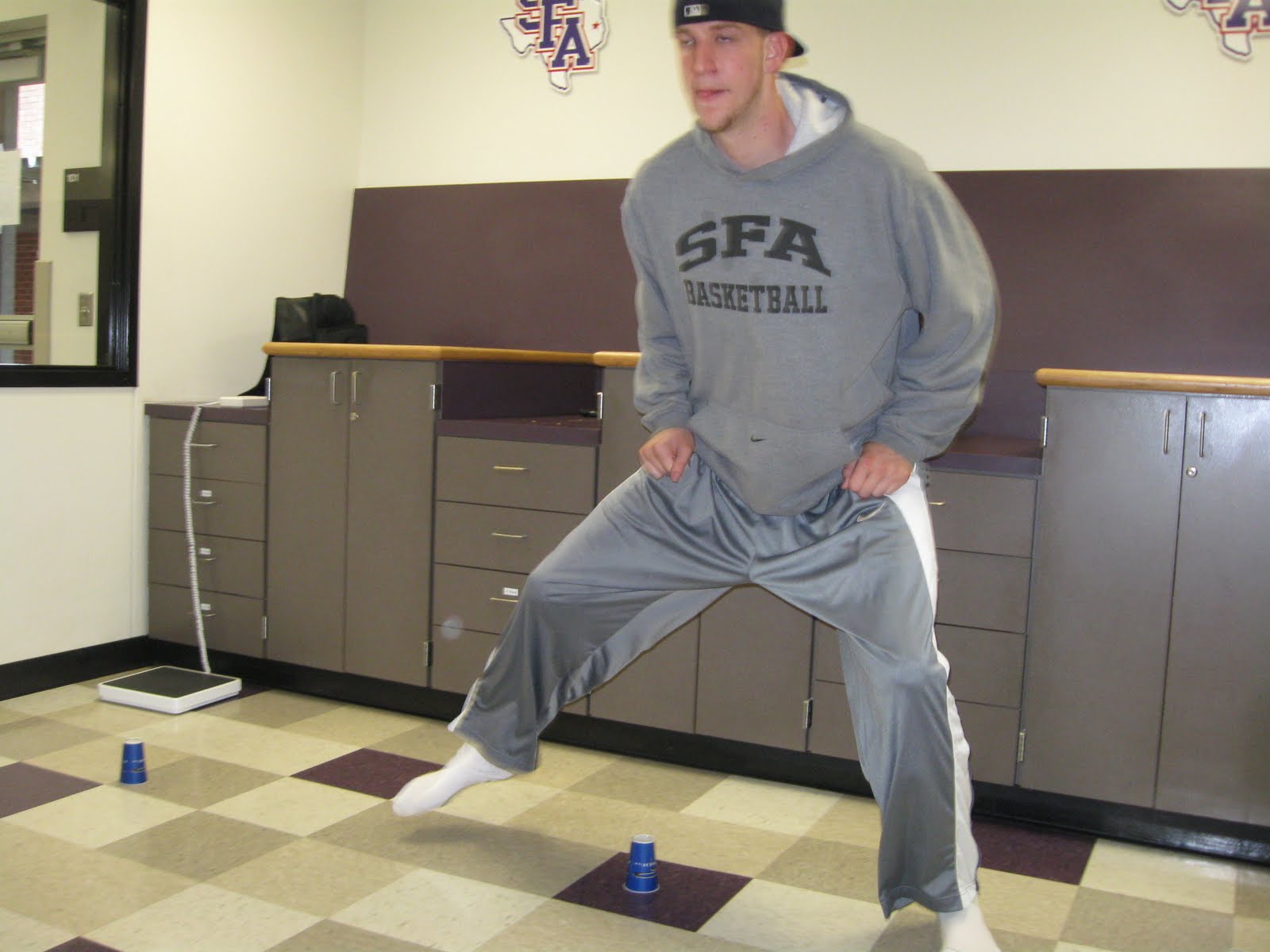
6. Dynadisc Balance (6 x 30secs) - Although this may seem like a relatively easy exercise, it will be extremely difficult for someone with a lower extremity injury. There are various way to work with the Dynadisc, as well as, working with the progression in difficulty (one leg, no shoes, ball-toss, visual impairment, etc.) However, in this particular exercise with this athlete, whom really enjoyed challenges, the goal was for him to stand for :30 secs at a time without falling off. That's it! It's a great way to increase proprioception and balance. The position with the athletes' hip at 90 degrees is the correct position. Below, the athlete is intentionally holding a squat position.



7. Lateral Step Ups (6 x 30 secs) - This specific exercise is to increase the athletes' trust in their ability to shuffle sideways, and it is a great way to build confidence in basketball related moves. A great way to progress this exercise is to remove the visual angle, and instead of concentrating on the placement of their feet, have them look straight ahead of focus on another target. Use this technique only if the individual has mastered all other related exercises and you are confident they are prepared to progress.




8. Med Ball Squats (6 x 30 secs) - Similar to a wall squat, this exercise is performed while the athlete holds their squat position, with any type of ball between their legs proximal to the knee, and squeeze, or prevent the ball from falling. A variation of this exercise we utilized for progression is to add resistance to the object between their legs. In this case, we used a heavier ball. When our patient got really good, and showed good medial quad strength, I would apply pressure to the ball by hitting it from different angles, using varying amounts of strengths.


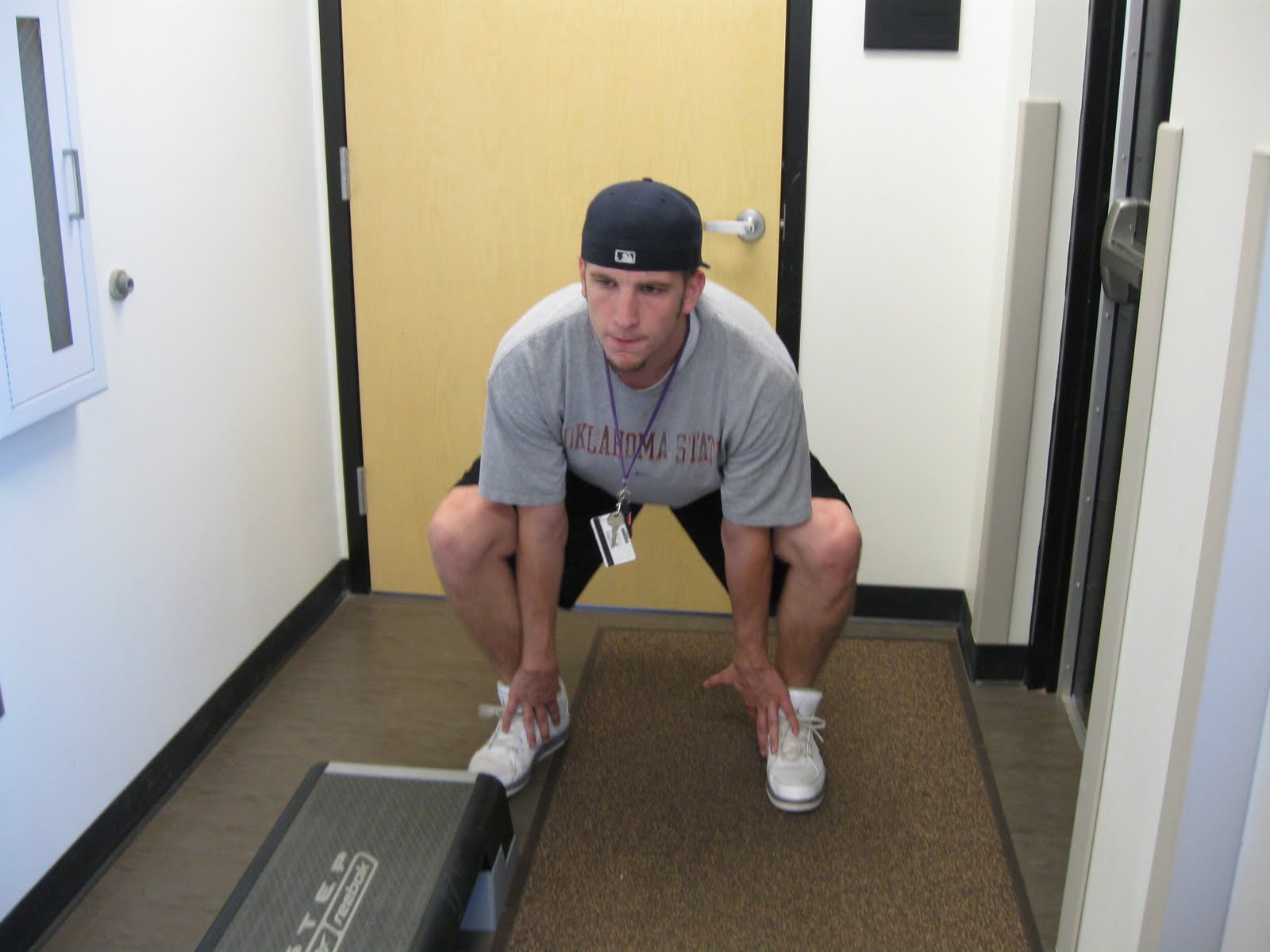
9. Floor Squats (3 x 12) - Having a relatively easy exercise is a huge benefit for the athlete's psyche, and physically, gives them a break from the more intense exercises. Typically, this exercise is performed after a few more rigorous ones. In the beginning, I like to have the athlete perform the squats in front of a mirror for visual feedback. Once they become good enough, I take away the visual aid, and then, the target becomes (as you can see in the picture) the inner soles of his shoes.
Plyometrics (3 x 15) - Plyometrics are an easy form of exercises to train athletes, and also, they are great for patients who are further along in their respective program. With our athlete being a basketball player, naturally, he wanted to get back to jumping, so this was an obvious drill. We simply used a jump rope and set it at a specific height. Here, he is jumping laterally, but this can be progressed by having them jump in different directions.



Jump Twist - Here, our patient is performing an exercise that will increase confidence using his knee, and help in regaining the specific level of athletic performance that he was used to. The important element here is landing. We want to focus on a controlled landing in which he does not wobble, or come down too hard, all the while working accessory and stabilizing muscles.



Exercise Ball Squats - This is an exercise that focuses on generating power and maintaining stability.



Reverse Total Gym (3 x 15) - This is the only exercise performed with a machine.

All the above exercises are advanced level exercises, in other words, are not recommended for acute injuries, or injuries still in the beginning stages of healing. A thorough evaluation should completed upon initial exercise prescription, also before progressing to more difficult exercises.